INTRODUCTION
Dermatoglyphics is the study of epidermal ridges and their configurations on the fingers, palms, and soles.[1] The term 'dermatoglyphics' is derived from two Greek words - 'derma', which means skin, and 'glyphae', which means carve. The term was coined by Cummins and Midlo in 1926.[2]
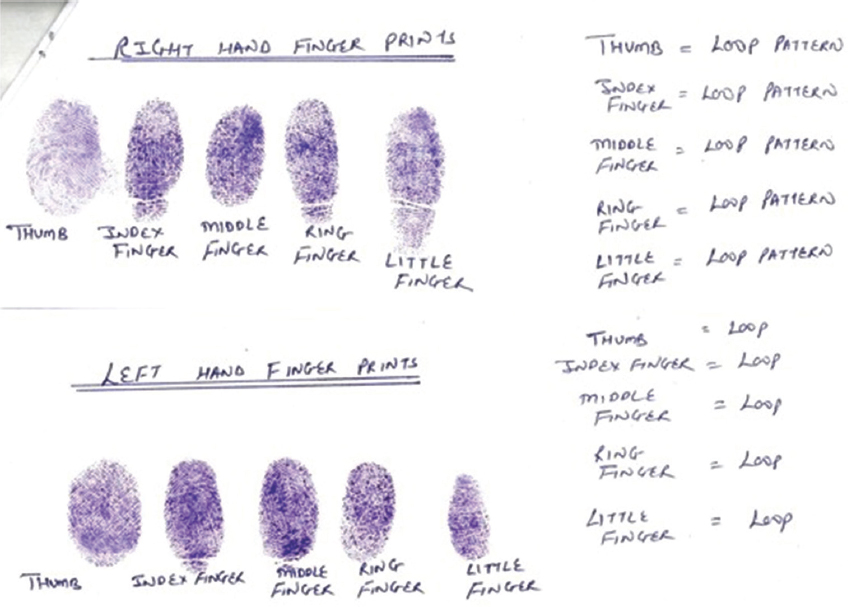
Dermal ridges begin to appear during the 12th week of intrauterine life and are completed by the 24th week of intrauterine life.[3,4] Thereafter, they remain constant, except for the change in their sizes. These dermal patterns and orodental structures embryologically develop during the same period. The three major patterns of fingerprints include arch, loop, and whorl patterns [Figure 1]. In the field of dentistry, the association of dermatoglyphics has been studied in precancerous and cancerous lesions in the oral cavity, dental caries, and dental anomalies such as cleft lip and palate and malocclusion.[5,6]

Figure 1. Fingerprint patterns
Malocclusion is a frequently reported oral condition that can be avoided, stopped, and fixed. The first step in preventing it is to be aware of the chance of developing malocclusion. Early identification of malocclusion is crucial for the best application of preventive and interceptive orthodontics.
Furthermore, relation of dermatoglyphics with dental occlusion is studied due to the fact that after the complete formation of dermal ridges, there is no change in their shape and remain in position throughout a person’s life. Thus, the present study was undertaken to ascertain the reliability of dermatoglyphics as a predictive tool for malocclusion to apply preventive and interceptive orthodontics to the high-risk groups. The purpose of the study was to study the relation of dermatoglyphics with skeletal class I normal occlusion, skeletal class II malocclusion, and skeletal class III malocclusion types in children of 12–14 years.