SUBJECTS AND METHODS
An institutional ethics committee approved this prospective two-group experimental study. Split mouth treatment was performed on 16 patients; 18–22 years old with healthy periodontium, good oral hygiene, and whose treatment plan included implant placement between mandibular 1st molar and 2nd premolar was chosen for this study from the department with patients’ informed consent. To eliminate the errors that could compromise the success of implant placement and the quality of the implant stability quotient (ISQ) reading and a stent was made out of 0.019 × 0.025” stainless steel for implant implantation. The stent’s entire length (from the bracket location) was limited to 9 mm, and its loop was 4 mm in diameter. The micro-implant was positioned 7 mm above the alveolar crest. The mesial and distal horizontal legs were ligated to the premolar bracket and molar tube respectively [Figure 1] after stent engagement, the area of the micro implant insertion was cleaned with povidone-iodine. A topical anesthetic was applied. With full retraction of the soft tissue, 0.5 ml of anesthetic solution (Lignocaine with adrenaline) was infiltrated in the mucosa. The insertion site was then evaluated with a probe to check if the area was anesthetized. This also serves as a visual marker for inserting the micro implant.

Figure 1: Stent engaged into premolar bracket and molar tube
Next, the titanium grade V self-drilling micro-implants of diameter 1.5 mm and length 6 mm[24] [Figures 2 and 3] were inserted in such a way as to obtain maximum insertion depth and an angulation of 90°. An intraoral periapical radiograph was taken to ensure that the micro implant angulation is satisfactory and to confirm that the adjacent roots were not injured [Figure 4].

Figure 2: Micro-implant of length 6 mm and diameter 1.5 mm

Figure 3: Micro-implant placed between 45 and 46
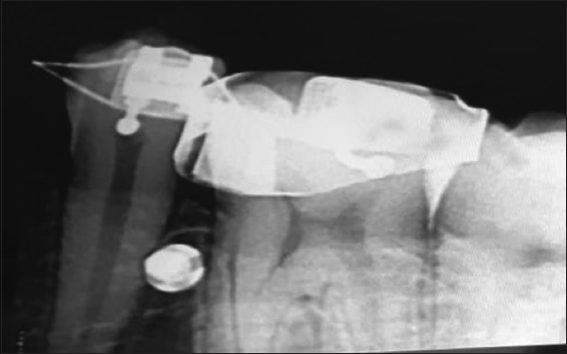
Figure 4: IOPA after micro- implant insertion. IOPA: Intraoral periapical radiograph
Laser irradiation
The irradiation site was selected by blind sampling. Sixteen envelopes, each containing eight letters RIGHT and eight letters LEFT, were prepared and kept by the nurse (who was not involved in the study). Each candidate voluntarily chose a sealed envelope, gave it to the nurse, and the nurse opened the envelope. He then informed the operator that the laser used in the procedure was a multimode GaAs diode laser with a wavelength of 980 nm. The output power was 0.5-10W, adjustable in the frequency range of 1-20KHz, and the body input voltage was DC12V~19V.
In the experimental group, implant site was irradiated with soft-tissue laser after placement, and in the control group, implant site was not irradiated with soft-tissue laser [Figure 5].
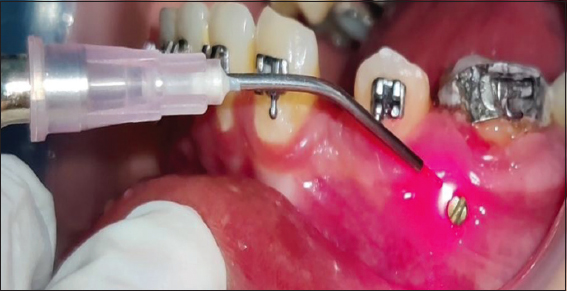
Figure 5: LLLI around the implant. LLLI: Low level laser irradiation
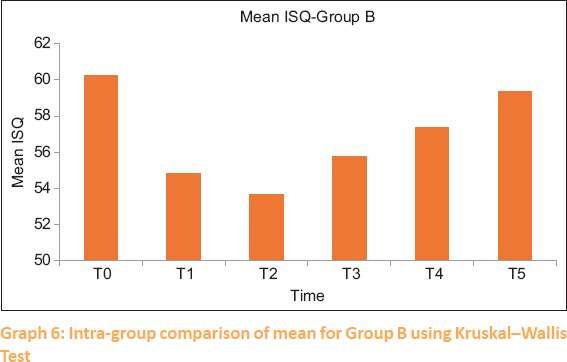
Resonance frequency analysis was used to gauge the implant’s stability. The principle for RFA assessment is the detection of the mini magnet embedded in the aluminum housing of an implant head, known as a smart peg [Figure 6]. The main unit of assessment is the resonance frequency emitted by the magnet. Because no Smart Pegs available are suitable for the orthodontic mini-implants a customized connector will be used for attachment between the two. The readings were recorded(T0) after insertion, (T1) 24 hours after insertion, (T2) 2 weeks after insertion, (T3) 4 weeks after insertion, (T4) 6 weeks after insertion, (T5) 8 weeks after insertion. Mean values were calculated for all six (3 in mesiodistal and 3 in occlusogingival directions) readings and that will be the overall ISQ value for each micro implant at each time [Figures 7-9]. The higher the ISQ values the greater will be the stability and hence the optimal loading time.

Figure 6: Smart Peg and customized connector engaged with the micro-implant head

Figure 7: ISQ reading in occluso-gingival and mesio-distal direction Implant Stability Quotient ISQ (No-55)
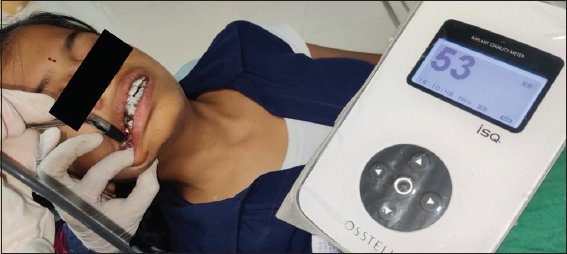
Figure 8: ISQ reading in occluso-gingival and mesio-distal direction Implant Stability Quotient ISQ (No-53)

Figure 9: ISQ reading in occluso-gingival and mesio-distal direction Implant Stability Quotient ISQ (No-52)