MATERIALS AND METHODS
The Department of Conservative Dentistry and Endodontics at the Post Graduate Institute of Dental Education and Research at the Indira Gandhi Institute of Medical Sciences in Patna, Bihar, India, was where this study was carried out. The study was conducted in accordance with the Declaration of Ethical Criteria for Medical Research Involving Human Participants in line with the Declaration of Helsinki, after independent peer review and approval by the Institutional Ethical Committee, before commencement. Following a thorough explanation of the treatment procedure in accordance with the patient information sheet, written informed consent was acquired from the patient (or parent, if the patient was younger than 14 years of age). The treatment outcome based on clinical and radiographic criteria was assessed by calibrated examiners. Patients of both groups were recalled for follow-up examinations after the first intervention at 6 and 12 months for the 1st year, and every year thereafter until the end of the study.
Inclusion criteria
-
Patients having maxillary anterior nonvital, immature teeth with open apex/apices with or without radiographic evidence of periapical lesion
-
Involving only occlusal surface, should not be tender to percussion
-
Ideal periodontal probing depth of 2–3 mm
-
The absence of furcation radiolucencies and periapical pathology were included in the present study
-
Radiographic evidence of deep caries proximal to the pulp chamber with no evidence of periodontal ligament thickening/widening.
Exclusion criteria
-
History of any systemic conditions such as diabetes, blood dyscrasias, patients on immunosuppressants, patient with bleeding disorder, platelet count <150,000/mm, 3 Asthmatic which could compromise the healing response
-
Root Fracture and symptomatic teeth (history of spontaneous pain) and nonrestorable teeth
-
Radiographic evidence of periapical changes or pathology
-
Negative response to pulp sensibility testing
-
Tooth not conducive for rubber dam isolation
-
History of the previous restoration in the tooth under consideration for pulp capping
-
Periodontally compromised teeth and patients with unsatisfactory oral hygiene maintenance and
-
Pregnant and lactating females
-
Patient not willing to participate in the study.
Treatment methodology
Patient’s medical, dental history, demographic, and socioeconomic data were collected. Intraoral examination was performed by a principle investigator. Pulpal and periradicular status was assessed through percussion, palpation, thermal, and electric pulp tests (Diagnostic unit; Sybron, Orange, CA). Periapical radiographic examination was performed using Rinn XCP devices (Rinn Corp, Elgin, IL) with Radio Visio Graphy (Vatech, Villa India, New Delhi, India).
Sample size calculation
The sample size was calculated using a free online available software G*Power (latest ver. 3.1.9.7; Heinrich-Heine-Universität Düsseldorf, Düsseldorf, Germany) for accessing Periapical healing (PAH) after 1 year. The calculation used an equivalence limit of 0.5, a standard deviation of 0.73, an alpha level of 0.05, an 85% power test, and a two-tailed hypothesis. In addition to it, in the present study, the sample size was also increased by 18% to compensate for any drop-out. This resulted in 18 roots each comprising of total 36 nonvital, immature, maxillary incisors and all were recruited for the study. Each patient was asked to select a chit from a box randomly representing the two groups with treatment protocols. The patients were categorized into two groups having eight carious roots each: Group I in which MTA Angelus (Angelus Indústria de Produtos Odontológicos S/A, Brazil) apexification was done without PRP into the canal and Group II had 8 roots where MTA apexification was supplemented with PRP carried on a collagen sponge (Metrogene – Septodont, France).
Group I: (Mineral trioxide aggregate apexification)The procedure of MTA Apexification was carried out as follows: Under Rubber dam isolation, access preparation was done in necrotic immature permanent teeth of all the 36 subjects. Canals were copiously irrigated with 2.5% sodium hypochlorite, and minimal instrumentation was done to prevent the weakening of the lateral dentinal walls. Triple antibiotic paste (TAP) was placed as an inter-appointment medicament in the dried canals, and the coronal access was sealed with intermediate restorative material for 4 weeks. During the visit of patients after 4 weeks under rubber dam isolation, TAP was removed from the canal using irrigation with 2.5% sodium hypochlorite. Canals were dried and following the procedure was carried out [Figure 1a-c].
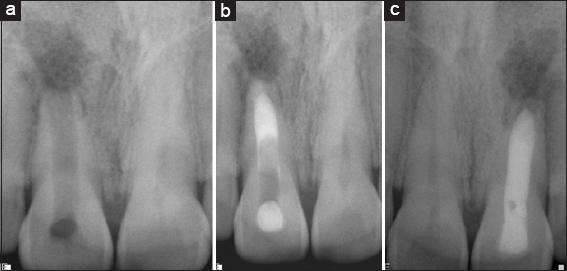
Figure 1: (a) Preoperative, (b) Mineral trioxide aggregate apexification, (c) Follow up 1 year
In Group I, MTA was placed in the canal using messing gun to form the 3–4 mm of apical plug. It was obturated using gutta-percha and AH Plus sealer. The tooth was permanently restored with adhesive restoration in the same visit.
Group II: (Mineral trioxide aggregate apexification + platelet-rich plasma on a collagen sponge)Under Rubber dam isolation, access preparation was done in necrotic immature permanent upper anterior of 18 patients (18 roots). In the cases subjected to revascularization, local anesthesia without a vasoconstrictor was administered at the first visit, with preparation of an access cavity, working length instrumentation, irrigation with 1.5%–2.5% sodium hypochlorite and 17% ethylenediamine tetraacetic acid, Canals were copiously irrigated with 2.5% sodium hypochlorite, and minimal instrumentation was done to prevent the weakening of the lateral dentinal walls. The TAP was placed as an inter-appointment medicament in the dried canals, and the coronal access was sealed with intermediate restorative material for 4 weeks. Moreover, patients were recalled after 4 weeks of treatment. In Group II PRP + collagen was introduced as a scaffold and pushed toward the apical area using endodontic pluggers and then MTA apexification was done using messing gun to form the 3–4 mm of the apical plug. It was obturated using gutta-percha and AH Plus sealer. The tooth was permanently restored with adhesive restoration during the same visit [Figure 2a-c].
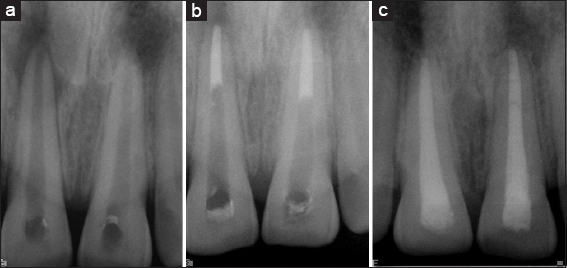
Figure 2: (a) Preoperative, (b) Mineral trioxide aggregate + Platelet rich plasma, (c) 1 year follow-up
Platelet-rich plasma preparation
It was done in a simple, tabletop laboratory centrifugation machine (Lab Care, LB-DCM8 India). 8.5 mL of whole blood was drawn by venipuncture of the antecubital vein. It was then collected in a 10 mL sterile glass tube with an anticoagulant (Acid Citrate Dextrose) in it. After 1st centrifugation at 2400 rpm for 10 min (soft spin), three separate layers were seen in the tube. After that, the PRP, soaked on a collagen sponge was introduced into the root canal and taken to the apical part of the canal and MTA apical plug was placed in the same appointment. In both the experimental groups, resin-modified glass ionomer cement was placed extending 3–4 mm in the canal. The access cavity was sealed with composite (Clearfil Majesty, Kuraray Medical Inc., Tokyo, Japan) during the same visit. Patients were kept on the follow-up of 6 and 18 months. Both clinical and radiographic evaluation was done at each follow-up visit. Clinically relief of symptoms such as pain, swelling, and resolution of sinus was evaluated and on radiograph healing of periapical lesion was noted.