CASE 1
A 24-year-old female patient reported to the Department of Conservative Dentistry and Endodontics, King George’s
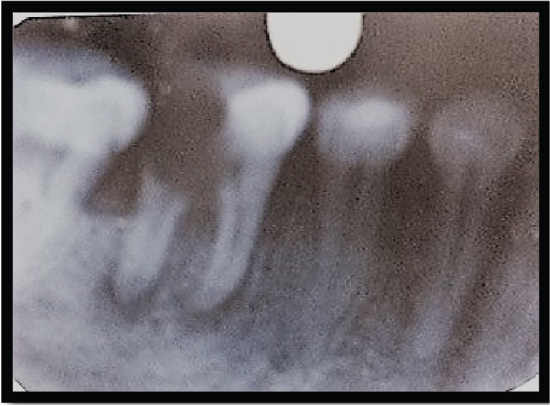
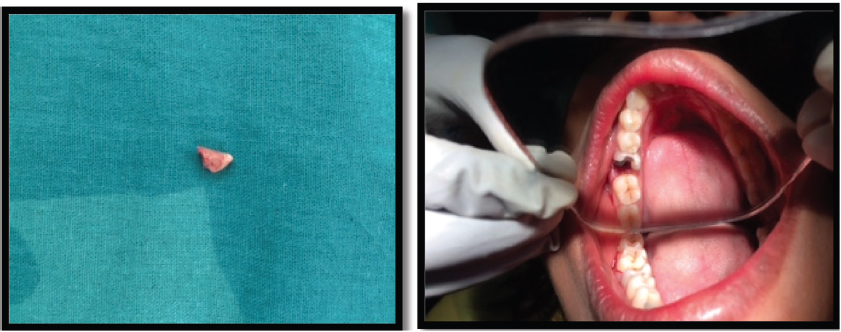
Medical College Faculty of Dental Sciences, Lucknow, with the complaint of pain in the left mandibular first molar (36) for 2-3 days. On examination, the tooth was found to be grossly carious [Figure 1]. The past medical history, as well as the past dental history of the patient, was nonsignificant. On radiographic examination, radiolucency was present in the distal root [Figure 2]. The mesial root was completely intact, but furcation was involved. It was decided that the distal root should be hemisected after the completion of endodontic therapy. Endodontic therapy was initiated with respect to the mesial root and completed in a single sitting. Canal cleaning and shaping were completed using 3% sodium hypochlorite (Septodent, France) along with 15% EDTA (Glyde, Dentsply, Tulsa, USA) and rotary file system Revo S (Micro-Mega, France). Obturation was performed by cold lateral compaction of gutta-percha [Figure 3]. Distal root hemisection was performed with a vertical cut method. The crown was cut with a tapered fissure carbide bur till the furcation was reached. After separation of both roots, the distal half was extracted [Figure 4]. The empty socket was thoroughly irrigated, and the flap was sutured. The patient was recalled for 1 month and evaluated for the healing of the extraction socket. After complete healing of the extraction socket, biomechanical preparation of the molar and premolar crown was done [Figure 5]. The reduced molar resembled a premolar in shape. A temporary bridge was seated during the healing and consolidation phase to prevent the drifting of the remaining root. Definitive restoration therapy was accomplished 6 weeks after hemisection [Figure 6]. A two-unit porcelain fused metal fixed partially replaced the distal root of the mandibular first molar and retainers on the second premolar and remaining part of the mandibular first molar. The interdental spaces are contoured so that hygiene can be accomplished with toothbrushes.
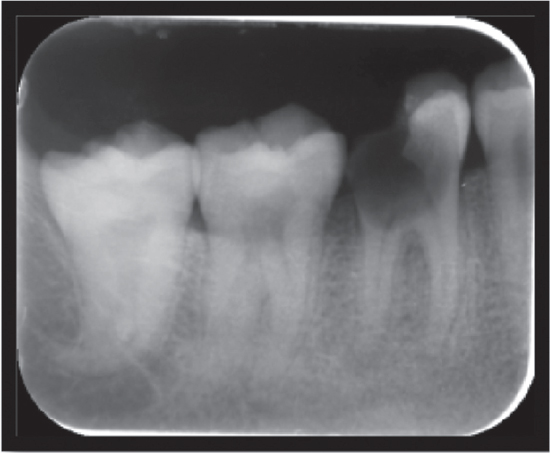
Figure 1. Grossly carious tooth

Figure 2. IOPAR showing radiolucency
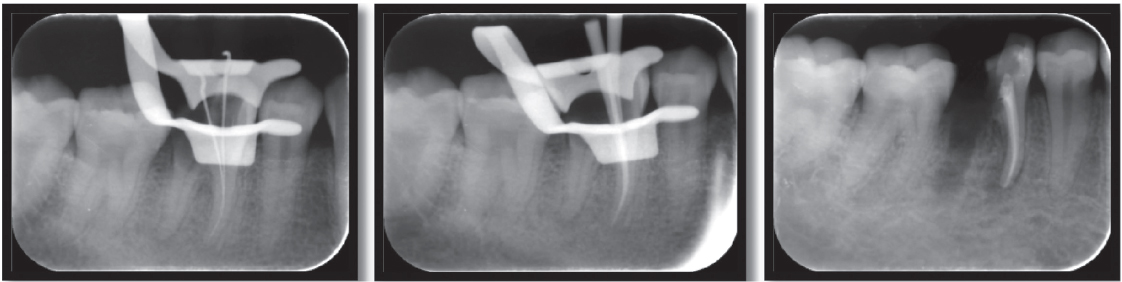
Figure 3. Steps of root canal treatment
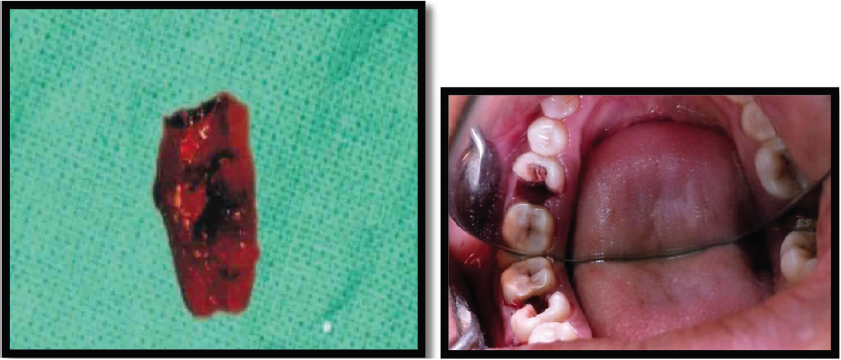
Figure 4. Hemisection of distal root

Figure 5. Preparation of crown

Figure 6. Post-Op 06 weeks