CASE REPORT
Case 1
A 24-year-old female patient reported to the Department of Conservative Dentistry and Endodontics at King George Medical College, Lucknow, with the chief complaint of small teeth in the upper front region and spacing between two upper front teeth. The patient’s medical history is not significant. Intraoral examination revealed the presence of midline spacing using a vernier caliper between maxillary central incisors (~2.5 mm) and peg-shaped lateral incisors with short clinical crowns and thick fibrous tissue between the central incisors [Figure 1a and b]. No dental caries were observed in both clinical and radiographical examinations. The patient had good periodontal health and a stable intercuspal position, normal vertical and horizontal overlap, and canine-protected guidance. The treatment plan was made keeping in view that the patient would not be able to afford expensive treatment and was also not willing to come in for multiple visits. The financial circumstances, patient’s age, and requirements of quick results by the patient, along with the available treatment options, precluded two potential interventions: comprehensive orthodontics and porcelain veneers. Consequently, a treatment plan was developed to enhance the patient’s smile through the application of direct composite veneers, effectively addressing the misalignment of the teeth.

Figure 1. (a and b) Peg shape lateral incisors with short shape crown. (c and d) Showing thick fibrous tissue removed and follow up. (e and f) Isolation adjacent tooth and Post-procedure
The treatment protocol was designed to include the excision of extensive fibrous tissue, followed by gingival contouring, and subsequently the application of direct composite veneers. Before the procedure, written informed consent was secured from the patient. The initial step involved the removal of the thick fibrous tissue utilizing a diode soft tissue laser, operating at a power setting of 1.5 W, after the administration of lidocaine 2% with epinephrine 1/100,000 by the infiltration technique [Figure 1c]. The patient was recalled after 1 week after healing the gingival [Figure 1d]. On the next visit, first, shade selection was done, and an A1 shade of Vita guide was selected for the teeth to be restored. Minimal preparation was done with diamond bur (#2135F; KGSorensen Indústria e Comércio Ltda, Barueri, SP, Brazil). Isolation of the operating area was achieved with cotton rolls as the patient was experiencing gagging with the rubber dam. The preparation was etched - with 37% phosphoric acid for 30 s, rinsed with water, and air-dried. The adjacent tooth was isolated using Teflon tape [Figure 1e]. A single layer of bonding agent (Prime & Bond® NT™, Dentsply Caulk) was applied and cured for 20 s with an LED composite curing unit. A thin layer of the nano-hybrid composite (Tetric N Ceram, Ivoclar Vivadent) was then incrementally applied to the tooth surface and light-cured for 40 s. Following this, the tooth was shaped, finished, and polished using a Super Snap mini kit (Shofu) [Figure 1f]. After completing the procedure, oral hygiene instructions were provided to the patient. The patient was scheduled for follow-up appointments at 1 week, 1 month, and 6 months post-procedure.
Case 2
A 26-year-old female patient presented with a primary concern regarding a smaller tooth located in the upper anterior region, as well as the presence of spacing between two upper anterior teeth. The patient reported no significant family or medical history. Intraoral examination revealed peg-shaped upper right permanent lateral incisors. Midline diastema was present between both the central incisors of 1 mm [Figure 2a and b]. The patient had good periodontal health. A radiographic examination indicated the presence of a peg-shaped lateral incisor with a normal root length. Prior to initiating the procedure, a palatal silicone putty index (DMG America) was fabricated [refer to Figure 2c]. This index served as a guiding tool for the application of the initial palatal composite layer. The restoration of the peg-shaped lateral incisor and the midline diastema was accomplished using direct resin composite veneers, following the procedure outlined in Case I [see Figure 2d]. Comprehensive oral hygiene instructions were provided, and the patient was scheduled for follow-up appointments at 1 week, 1 month, and 6 months post-treatment [Figure 2e and f].
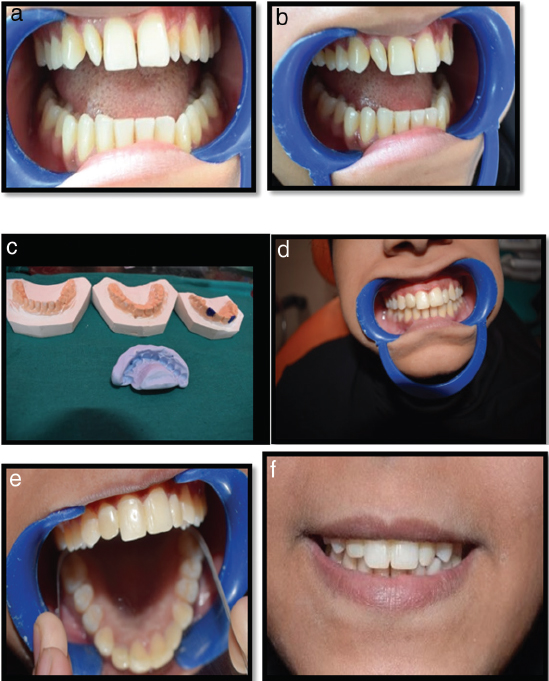
Figure 2. (a and b) Midline diastema. (c and d) Fabrication of palatal silicone putty and restoration with direct composite veneers. (e and f) Post treatment follow up 1 month and 6 month
DISCUSSION
Establishing a patient’s natural dental aesthetics is a critical aspect of contemporary dentistry, alongside considerations of function and phonation. Abnormalities in the color, shape, and positioning of anterior teeth can lead to significant esthetic challenges for patients. In Case 1, a thick fibrous tissue was identified between the central incisor and the permanent right lateral incisor, while the left lateral incisor presented as peg-shaped. Consequently, an intervention was undertaken to excise the fibrous tissue and close the midline space, adhering to the principles of the golden proportion. Additionally, the right maxillary canine was shaped to resemble that of the lateral incisor. This approach in Case 1 demonstrated various advantages, including being noninvasive, esthetic, efficient, and provides prompt results and minimal patient compliance requirements.[3,7,8]
Direct composite veneers are a more conservative option to porcelain because with the use of microhybrid and nano- hybrid composites, the finishing and polishing of these restorations look like porcelain veneers. The success rate of direct composite and durability of these materials depends on patient habits like smoking or drinking dark-colored liquids, which alter the color of the teeth.[3] Direct composites do not have nature of brittleness and abrasive wear as compared to porcelain crowns.[9,10] The presence of a midline diastema or spaces in between anterior teeth can be a major esthetic concern for patients. There are various treatment options available for diastema closure like orthodontic movement and prosthodontic treatment. Among these, the use of direct resin restorations seems to be a conservative, cost-effective, and more practical option.[11]
Direct composite veneers are a more conservative option compared to porcelain veneers. With the use of microhybrid and nano-hybrid composites, the finishing and polishing of these restorations can closely resemble that of porcelain veneers. The success rate and durability of direct composites depend significantly on patient habits, such as smoking or consuming dark-colored beverages, which can alter the color of the teeth.[3] Unlike porcelain crowns, direct composites are less brittle and experience less abrasive wear.[19,10] Patients often find the presence of a midline diastema or spaces between their anterior teeth to be a significant esthetic concern. There are several treatment options available for diastema closure, including orthodontic movement and prosthodontic treatments. Among these, direct resin restorations are considered more conservative, cost-effective, and practical.[11]
In this case report, the patient’s expectations were not only met but exceeded through the use of conservative direct composite restorations, demonstrating the efficacy and precision of this approach in enhancing patient satisfaction.
CONCLUSION
Composite resin restorations for midline diastemas and peg-shaped laterals demonstrate commendable clinical acceptance and retention when all established protocols are meticulously adhered to, employing the appropriate clinical techniques. This aspect of esthetic dentistry represents one of the rare opportunities for patients to effectively assess the quality of the work performed.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form, the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
1. Neeraj K. Veneer in restorative dentistry. Asian J Oral Health Allied Sci 2012;2:17-25. [Google Scholar]
2. Rathi S, Dhannawat P, Gilani R, Vishnani R. A multidisciplinary aesthetic treatment approach for peg lateral of the maxillary incisors. Cureus 2022;14:29184. [CrossRef] [Google Scholar]
3. Izgi A, Ayna E. Direct restorative treatment of peg-shaped maxillary lateral incisors with resin composite:A clinical report. J Prosthet Dent 2005;93:526-9. [CrossRef] [PubMed] [Google Scholar]
4. King S, Sood B, Ashley MP. Practical advice for successful clinical treatment with resin-bonded bridges. Br Dent J 2023;235:503-9. [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
5. Goyal A, Nikhil V, Singh R. Diastema closure in anterior teeth using a posterior matrix. Case Rep Dentis 2016;2016:2538526. [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
6. Korkut B, Yanikoglu F, Gunday M. Direct composite laminate veneers:Three case reports. JODDD 2013;7:105-11. [Google Scholar]
7. Al-Rubayee MA. Median diastema in a college students sample in the Baghdad city. Med J Babylon 2013;10:400-6. [Google Scholar]
8. Calheiros-Lobo MJ, Calheiros-Lobo M, Pinho T. Esthetic perception of different clinical situations of maxillary lateral incisor agenesis according to populations with dental and non-dental backgrounds:A systematic review and meta-analysis. Dent J (Basel) 2023;11:105. [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
9. Sonar PR, Panchbhai AS, Vaidya S. Anterior aesthetic rehabilitation for midline diastema closure with veneers:A case report. Cureus 2023;15:49704. [CrossRef] [Google Scholar]
10. Farah RI, Al-Haj Ali SN, Alharbi A, Alresheedi B. Straightforward replication of digital wax-up design into direct composite resin restorations in adolescents using a custom 3-dimensionally printed index. Restor Dent Endod 2024;49:36. [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
11. Sabnis R, Vasunni GK, Mahale P, Kamble GT. Esthetic conservative management of interdental spaces using direct composite resin restorations- A case report. IOSRJ Dent Med Sci 20142014;13:109-12.[CrossRef] [Google Scholar]