CASE REPORT
A 45-year-old conscious and well-oriented male was presented to the emergency department with painful swelling in the left cheek and a wound dressing in the left submandibular region, which had been in place for two hours [Figure 1]. The patient exhibited positive responsiveness to verbal commands and initially received first aid treatment at a rural health facility. The patient demonstrated positive responsiveness to verbal commands and initially received first aid treatment at a rural health facility. The patient’s medical history revealed that the trauma was a result of contact with a fragment of a grinding wheel rotating at high speed. Furthermore, upon extraoral examination, a laceration measuring approximately 4 × 2 cm was identified in the left body-angle region, affecting the skin and the underlying platysma muscle. A substantial clot and green grinding disc fragments were observed within the wound. The patient exhibited limited ability to rotate his head to the left. Intraorally, no discrepancies or instability in occlusion were noted, and there was no active bleeding at the injury site. A computed tomography (CT) scan was advised to the patient. Skull base and vertebrae fracture were ruled out. It revealed multiple radiopaque foreign objects scattered all over the submandibular and the retromandibular region, with the largest piece (2.2 × 0.5 cm) presented posterior to the left ramus of the mandible inferior to the left parotid gland. It also revealed a hematoma of 7 × 5 cm in size about the left mandible body and ramus region which corroborated the clinical finding [Figure 1]. The case was taken as an emergency. Wound debridement under GA was the treatment plan decided. The incision was made by widening the existing laceration present extraorally. The hematoma was carefully removed with the help of gauze. Foreign bodies were visualized after the hematoma removal, especially the ones present in the retromandibular region. The wound was thoroughly explored, and disc fragments were removed. The larger piece was removed using a curved artery taking care not to damage any adjacent vital structures [Figure 2]. There was a presence of powder of the foreign body which was cleared out using copious saline irrigation. Closure was done in multiple layers using 3-0 vicryl sutures. Aggressive pre- and post-operative antibiotic coverage was given. Extraoral pressure bandage was given to obliterate any dead space. The post-operative period was uneventful. The patient was followed up for the next 3 months with no further complaints [Figure 3].
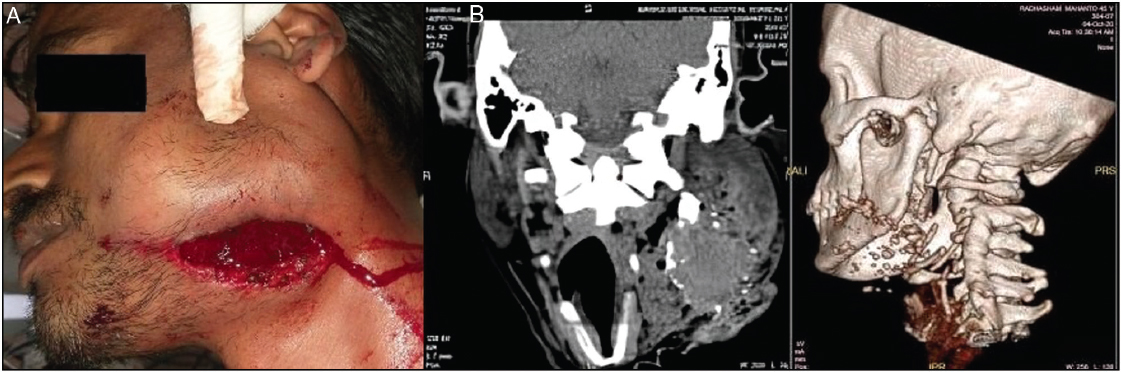
Figure 1: (A) Pre-operative picture of the patient. (B) Pre-operative CT scan
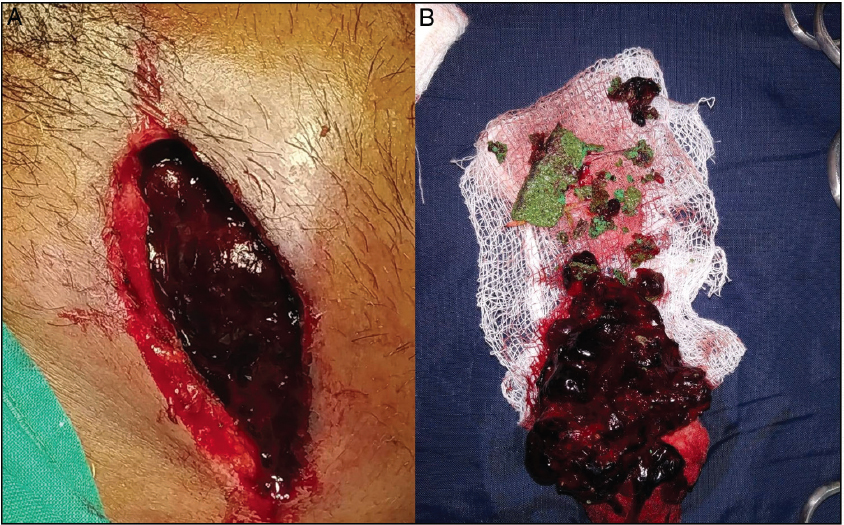
Figure 2: (A) Wound debridement. (B) The presence of hematoma and glass piece

Figure 3: (A) Post-operative picture of the patient. (B) Post-operative CT scan