RESULTS
Groups A and B had mean ages of 26.20 ± 6.01 and 27.15 ± 6.21 years, respectively. A t test showed similar ages between the two groups (P > 0.05; 26.20 ± 6.01 vs. 27.15 ± 6.21, t = 0.49; P = 0.626) [shown in Table 1]. In Group A, the dry socket was present in three subjects (15.0%), whereas in Group B, it was present in one subject (5.0%). Comparing the dry socket proportion (Absent A/P Present) of two groups, χ2 test revealed similar (p > 0.05) dry socket proportion in two groups (Absent/Present: 17/3 vs. 19/1 χ2 = 1.11; P = 0.292) [shown in Table 1].
Table 1: Basic characteristics of two groups
| Characteristics | Group A (n = 20) | Group B (n = 20) | t/χ2 value | P value |
|---|---|---|---|---|
| Age (years) | 0.49 | 0.626 | ||
| Mean ± SD | 26.20 ± 6.01 | 27.15 ± 6.21 | ||
| Range (min–max) | (19–40) | (19–42) | ||
| Gender | 0.40 | 0.525 | ||
| Males | 10 (50.0%) | 12 (60.0%) | ||
| Females | 10 (50.0%) | 8 (40.0%) | ||
| Dry socket | 1.11 | 0.292 | ||
| Absent | 17 (85.0%) | 19 (95.0%) | ||
| Present | 3 (15.0%) | 1 (5.0%) |
Swelling
The swelling levels of the two groups before (day 1) and after (days 2 and 7) treatments are summarized below. The average swelling level increases after the treatments and decreases after 7 days, almost returning to initial levels. The change was higher in Group B than in Group A. Comparing the average swelling levels within each group, they increased significantly from day 1 to day 2 and decreased significantly from day 2 to day 7. However, there was no significant difference between day 1 and day 7 for both groups [shown in Tables 2–4].
Table 2: Pre and postswelling levels (mean ± SD) of two groups over the periods
| Groups | Day 1 | Day 2 | Day 7 |
|---|---|---|---|
| Group A | 11.57 ± 1.16 (9.25–14.15) | 12.49 ± 1.09 (10.60–15.80) | 11.58 ± 0.93 (10.30–14.00) |
| Group B | 11.89 ± 0.65 (10.15–12.95) | 12.90 ± 1.39 (11.60–16.40) | 12.06 ± 0.55 (11.30–12.95) |
Table 3: For each group, the significance (P value) of the mean difference of swelling levels with the groups (i.e., between periods) by Tukey test
| Comparisons | Group A | Group B |
|---|---|---|
| Day 1 vs. day 2 | P < 0.001 | P < 0.001 |
| Day 1 vs. day 7 | 1.000 | 1.000 |
| Day 2 vs. day 7 | P < 0.001 | P < 0.001 |
Table 4: For each period, the significance (P value) of the mean difference of swelling levels between the groups by Tukey test
| Periods | Comparisons (Group A vs. Group B) |
|---|---|
| Day 1 | 0.914 |
| Day 2 | 0.794 |
| Day 7 | 0.655 |
Trismus
For each group, comparing the mean trismus levels within the groups (i.e., between periods) [Tables 5 and 6 and Figure 1], the trismus levels in both Groups A and B increased significantly (P < 0.001) at day 2 compared with day 1, whereas decreased significantly (P < 0.001) at day 7 compared with day 2. However, in both groups, the mean trismus levels did not differ (P > 0.05) between day 1 and day 7 that is, found to be statistically the same [shown in Tables 5 and 6; Figure 1].
Table 5: Pre and post trismus levels (mean ± SD) of two groups
| Groups | Day 1 | Day 2 | Day 7 |
|---|---|---|---|
| Group A | 26.50 ± 3.22 (22–36) | 18.90 ± 2.25 (16–26) | 26.00 ± 2.73 (22–34) |
| Group B | 25.83 ± 1.75 (22–28) | 19.98 ± 1.46 (18–24) | 25.85 ± 1.69 (22–28) |
Table 6: For each group, the significance (P value) of the mean difference of trismus levels with the groups (i.e., between periods) by Tukey test
| Comparisons | Group A | Group B |
|---|---|---|
| Day 1 vs. day 2 | P < 0.001 | P < 0.001 |
| Day 1 vs. day 7 | 1.000 | 0.852 |
| Day 2 vs. day 7 | P < 0.001 | P < 0.001 |
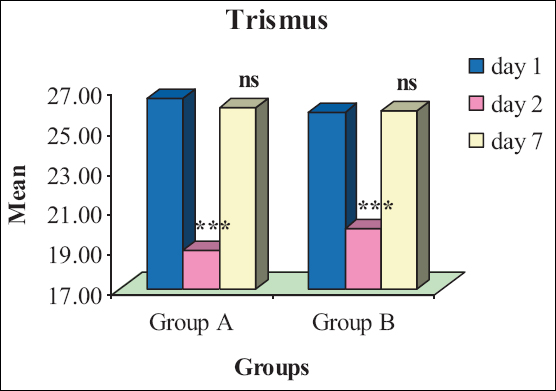
Figure 1: For each group, comparative trismus levels within the groups (i.e., between periods). nsP > 0.0.05 or *** P < 0.001 as compared to day 1
Similarly, for each day, comparing the mean trismus levels between the groups [Table 7], the trismus levels at all periods did not differ (P > 0.05) between the two groups that is, found to be statistically the same.
Table 7: For each period, the significance (P value) of the mean difference of trismus levels between the groups by Tukey test
| Periods | Comparisons (Group A vs. Group B) |
|---|---|
| Day 1 | 0.934 |
| Day 2 | 0.667 |
| Day 7 | 1.000 |
Pain
The pain levels before and after treatments for the two groups are summarized in Tables 8 and 9. Both groups experienced an increase in mean pain level after treatment (day 2), followed by a decrease after 7 days, almost returning to the initial levels (day 1).The change was more significant in Group B compared to Group A.
Table 8: Pre and postpain levels (Mean ± SD) of two groups over the periods
| Groups | Day 1 | Day 2 | Day 7 |
|---|---|---|---|
| Group A | 0.35 ± 0.49 (0–1) | 4.60 ± 0.88 (4–6) | 0.45 ± 0.51 (0–1) |
| Group B | 0.40 ± 0.50 (0–1) | 6.60 ± 0.75 (6–8) | 0.60 ± 0.50 (0–1) |
Table 9: For each period, the significance (P value) of the mean difference of pain levels between the groups by Tukey test
| Periods | Comparisons (Group A vs. Group B) |
|---|---|
| Day 1 | 1.000 |
| Day 2 | P < 0.001 |
| Day 7 | 0.074 |
For each group, comparing the mean pain levels within the groups (i.e., between periods) [Tables 10 and 11], the pain levels in both Groups A and B increased significantly (P < 0.001) at day 2 compared with day 1, whereas decreased significantly (P < 0.001) at day 7 compared with day 2. However, in both groups, the mean pain levels did not differ(P > 0.05) between day 1 and day 7 that is, found to be statistically the same [Table 9 and Figure 2].
Table 10: For each group, the significance (P value) of the mean difference of pain levels with the groups (i.e., between periods) by Tukey test
| Comparisons | Group A | Group B |
|---|---|---|
| Day 1 vs. day 2 | P < 0.001 | P < 0.001 |
| Day 1 vs. day 7 | 0.996 | 0.919 |
| Day 2 vs. day 7 | P < 0.001 | P < 0.001 |
Table 11: Operating time levels (mean ± SD) of two groups
| Group A (n = 20) | Group B (n = 20) | t value (DF=38) | P value |
|---|---|---|---|
| 47.75 ± 9.81 (32–70) | 29.40 ± 4.89 (20–38) | 7.49 | P < 0.001 |
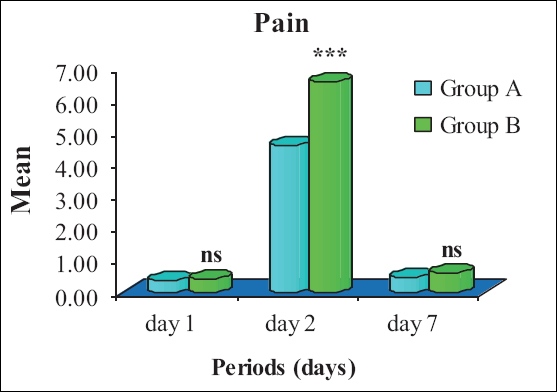
Figure 2: For each day, comparative pain levels between the groups
Operating time
The operating times of the two groups are summarized in Table 11 and also shown graphically in Figure 3. The operating time of Groups A and B ranged from 32 to 70 min and from 20 to 38 min, respectively, with a mean ± SD of 47.75 ± 9.81 and 29.40 ± 4.89 min, respectively. The mean operating time of Group B was comparatively lower than Group A. Comparing the mean operating time of the two groups, t test revealed significantly (P < 0.001) and 38.4% lower operating time of Group B compared with Group A (47.75 ± 9.81 vs. 29.40 ± 4.89, t = 7.49; P < 0.001).
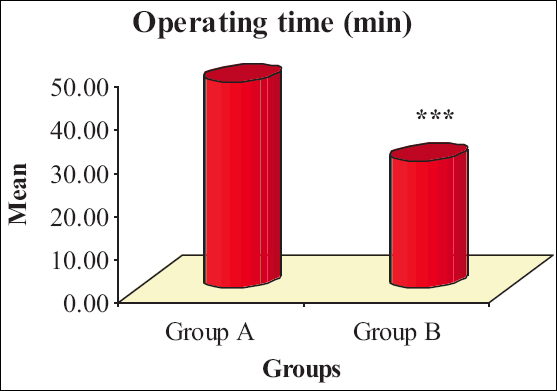
Figure 3: Mean operating time of two groups