RESULTS
A total of 7400 patients who reported to the outpatient department were screened, of which 291 were diagnosed to be affected with the recurrent aphthous ulcer, giving the overall prevalence of the disease to be 3.9% [Table 1]. Among 291 recurrent aphthous ulcer patients, 143 (49.1%) were male and 148 (50.9%) were female [Figure 1]. The prevalence of recurrent aphthous ulcers was 1.8% higher in females than males. The age of recurrent aphthous ulcer patients ranged from 1 to 80 years with a mean age of 25.10 years. The prevalence of recurrent aphthous ulcers was higher in lower age groups (11–40), accounting for 239, which was 82.1% of the total recurrent aphthous ulcer [Figure 2]. Interestingly, the prevalence of recurrent aphthous ulcers was found to decrease with an increase in age.
Table 1: Overall prevalence of recurrent aphthous ulcer
| Total patients screened (n=7400) | Number of patients, n (%) |
|---|---|
| Recurrent aphthous ulcer absent | 7109 (96.1) |
| Recurrent aphthous ulcer present | 291 (3.9) |
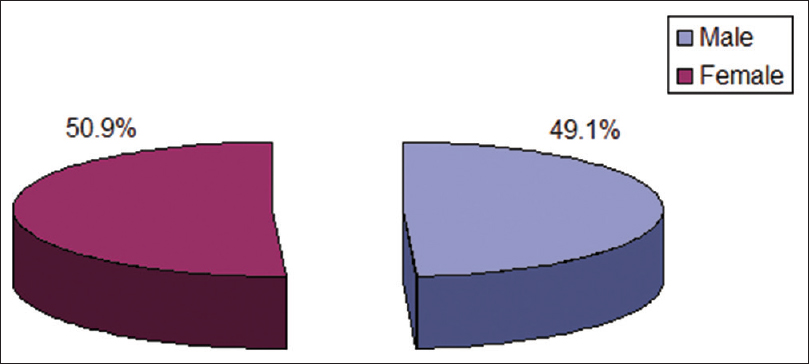
Figure 1: Prevalence of recurrent aphthous ulcer according to gender
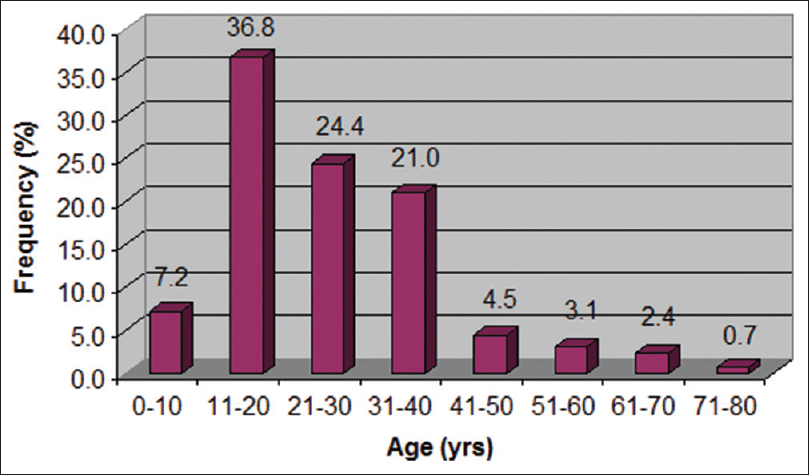
Figure 2: Prevalence of recurrent aphthous ulcer in different age groups
The prevalence of recurrent aphthous ulcers according to sites was 320, as 11 patients reported 29 more recurrent aphthous ulcers at multiple sites. According to the site, the prevalence of recurrent aphthous ulcer was maximum in the tongue (45.3%) followed by lower lip (34.1%), accounting together 79.4% of the total recurrent aphthous ulcer at different sites [Table 2 and Figure 3]. The prevalence of it was found minimum on the floor of the mouth (0.9%).
Table 2: Prevalence of recurrent aphthous ulcer according to age and sites
| Age (years) | Tongue (n=145), n (%) | Lower lip (n=109), n (%) | Upper lip (n=27), n (%) | Buccal mucosa (n=23), n (%) | Soft palate (n=13), n (%) | Floor of the mouth (n=3), n (%) | χ2 | P |
|---|---|---|---|---|---|---|---|---|
| 0-10 | 12 (8.3) | 9 (8.3) | 0 | 1 (4.3) | 1 (7.7) | 0 (0.0) | 21.19 | 0.968 |
| 11-20 | 55 (37.9) | 39 (35.8) | 10 (37.0) | 8 (34.8) | 2 (15.4) | 1 (33.3) | ||
| 21-30 | 30 (20.7) | 29 (26.6) | 8 (29.6) | 7 (30.4) | 4(30.8) | 1 (33.3) | ||
| 31-40 | 31 (21.4) | 24 (22.0) | 7 (25.9) | 4 (17.4) | 3 (23.1) | 1 (33.3) | ||
| 41-50 | 7 (4.8) | 3 (2.8) | 1 (3.7) | 1 (4.3) | 2 (15.4) | 0 | ||
| 51-60 | 5 (3.4) | 3 (2.8) | 1 (3.7) | 0 | 1 (7.7) | 0 | ||
| 61-70 | 4 (2.8) | 2 (1.8) | 0 | 1 (4.3) | 0 | 0 | ||
| 71-80 | 1 (0.7) | 0 | 0 | 1 (4.3) | 0 | 0 |
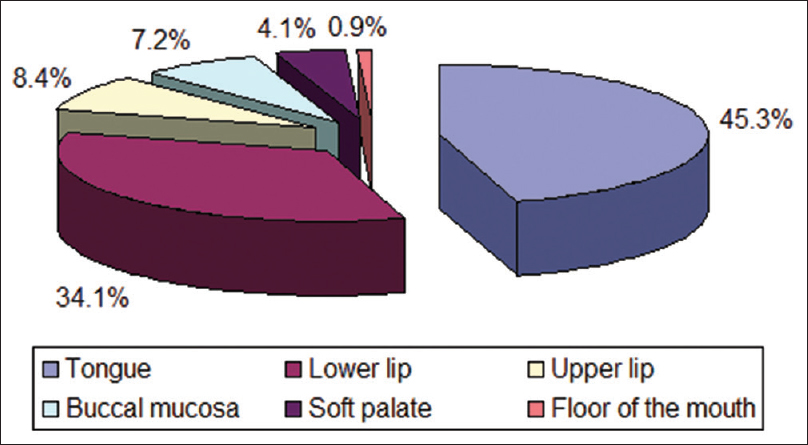
Figure 3: Prevalence of recurrent aphthous ulcer according to sites
The site-wise prevalence of recurrent aphthous ulcers in different age groups is summarized in Table 2 and also depicted in Figure 3. According to age, the maximum cases affecting tongue were seen in the second decade of life (37.9%), followed by the fourth (21.4%) and third (20.7%) decades of life. The second most affected was lower lip, again highest in the second decade of life (35.8%), followed by third (26.6%) and fourth (22.0%) decades of life. However, the Chi-square test showed an insignificant (P > 0.05) difference in the prevalence of recurrent aphthous ulcer between age and sites (χ2 = 21.19, P = 0.968), indicating a similar distribution of recurrent aphthous ulcer between age and sites.
Similarly, the prevalence of recurrent aphthous ulcers according to age and gender is summarized in Table 3 and also shown in Figure 3. In both genders, the prevalence of recurrent aphthous ulcers was higher in lower age groups (11–20 years) as compared to higher age groups (41–80 years). Like sites, the prevalence of recurrent aphthous ulcers also not differed (P > 0.05) between age and genders (χ2 = 8.12, P = 0.323), indicating a similar distribution of recurrent aphthous ulcers among age.
Table 3: Prevalence of recurrent aphthous ulcer according to age and genders
| Age (years) | Male (n=143), n (%) | Female (n=148), n (%) | χ2 | P |
|---|---|---|---|---|
| 0-10 | 8 (5.6) | 13 (8.8) | 8.12 | 0.323 |
| 11-20 | 46 (32.2) | 61 (41.2) | ||
| 21-30 | 35 (24.5) | 36 (24.3) | ||
| 31-40 | 34 (23.8) | 27 (18.2) | ||
| 41-50 | 8 (5.6) | 5 (3.4) | ||
| 51-60 | 5 (3.5) | 4 (2.7) | ||
| 61-70 | 5 (3.5) | 2 (1.4) | ||
| 71-80 | 2 (1.4) | 0 (0.0) |
DISCUSSION
Recurrent aphthous ulcer is the most common disease affecting the oral cavity. Many researchers have attempted to calculate its prevalence, but the results vary in different regions of the world, the range being from 5% to 66%.[9-11]
In the present study, the prevalence was found to be 3.93%. This, in comparison to the prevalence reported in other studies done in India, was found to be higher than reported in the South Indian population by Hegde et al. (1.9%)[12] and Mathew et al. (2.1%)[13] and in the Western population of Maharashtra as reported by Rajmane et al. (0.1%),[14] but the prevalence reported in this study was lower when compared to the findings of Patil et al. in North Indian population (21.7%).[15]
Worldwide also, the results of the epidemiological studies are greatly variable. It was estimated to be 40% in the United States of America,[16] 25.2% in Iran,[11] 25.5% in Turkey,[17] 1.4% in Brazil,[7] 28.2% in Iraq,[18] and 78.1% in Jordon.[19] Considerable variation is probably due to genetic factors, socioeconomic level, and lifestyle of individuals of the particular region studied.[20] In the present study, the overall prevalence was found to be higher in the female patients which was in accordance with the results of other researchers.[7,12,14,15,18,19] Ship et al. stated that higher prevalence in females was due to hormonal changes.[21] On the contrary, Rivera-Hidalgo et al. reported a higher prevalence in males.[22]
The maximum number of cases were reported in the second decade of life (36.76%) and then decreased with the advancing age. Ship et al.[21] and Natah et al.[23] also reported similar results. However, Abdullah18 and Okoh and Ikechukwu[24] found the maximum number of cases in the third decade of life, while Safadi[19] and Patil et al.[15] reported it to peak in the fourth decade of life. The most common site affected was found to be the tongue. Queiroz et al.[7] also reported tongue to be the most common site affected. Other studies have however reported buccal mucosa[14,19] to be the most common site. Abdullah reported lips and buccal mucosa to be the most common site.
CONCLUSION
Prevalence studies can be used to create and evaluate health-care policies in addition to detecting illness burdens in a population. Aphthous ulcers are prevalent mouth diseases that produce considerable discomfort and have a negative impact on patients’ quality of life. Despite this, the exact prevalence of recurring aphthous ulcers in India and around the world is unknown, and the data available are inconsistent. This study gives critical information on the occurrence of recurrent aphthous ulcers and their distribution in different age groups based on gender and site. Even without a proven etiology, it is also extremely important to identify factors associated with recurrence episodes to examine the potential risks of exacerbation of pain symptoms for each patient. More research like this is needed to achieve accurate disease data.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.