CASE SERIES
Case 1
Traumatic ulcer
A 58-year-old female reported with a chief complaint of frequent oral wounds on the right side of the tongue for 4 months. Presently, she complained of a painful oral wound on the right side of the tongue for 1 week. On examination, two predominant oral ulcers measuring 0.7 cm and 0.4 cm approximately were present in the tongue’s right lateral border in relation to #46 region [Figure 1a]. Two more healing ulcers were also present distal to the present ulcers connoting the frequent oral ulcerations. On palpation, the ulcers were tender and nonindurated in nature. No bleeding on palpation was present. Hard-tissue examination revealed a grossly carious root of #46, traumatizing the tongue. Based on the history and clinical findings, the patient was provisionally diagnosed with traumatic ulcers in the right lateral border of the tongue. The patient was prescribed topical analgesics and anti-inflammatory agents for symptomatic relief of pain caused by oral ulcers. Extraction of 46 was done under local anesthesia. The patient was reviewed after 2 weeks; there was complete healing of traumatic oral ulcers [Figure 1b].
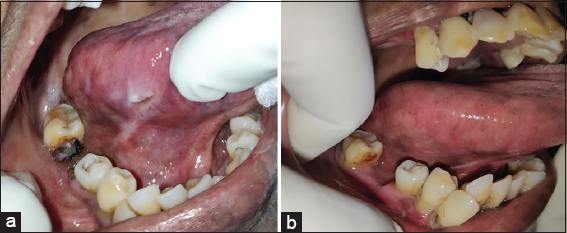
Figure 1: Traumatic ulcer of right lateral border of tongue – (a) Pretreatment. (b) Posttreatment
Case 2
Frictional keratosis
A 49-year-old male presented with the chief complaint of a sharp tooth impinging the tongue in the left side of the tongue. On examination, there was a white keratotic lesion of 1 cm × 0.5 cm present in the left lateral border of the tongue [Figure 2]. The hard-tissue examination revealed an attrited sharp cusp in relation to #36 which was traumatizing the left lateral border of the tongue. Based on the history and clinical findings, a provisional diagnosis of frictional keratosis was arrived. The occlusal grinding of the sharp cusp was done and the patient is under periodic follow-up.
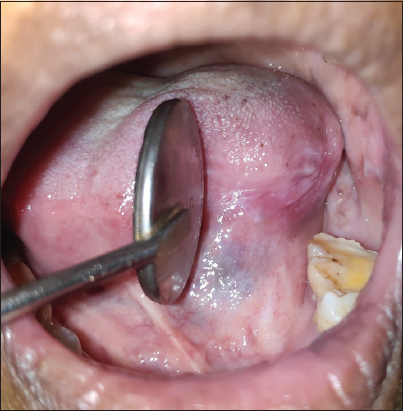
Figure 2: Frictional keratosis of left lateral border of tongue
Case 3
Traumatic fibroma
A 28-year-old female complained primarily of pain and swelling in the inner part of the left cheek region, noted over 3 weeks. In the beginning, the pain was gradual and worsened while eating. On examination, there was a solitary, well-defined sessile growth of 1.0 cm × 0.5 cm with surface ulceration present in the posterior buccal mucosa in relation to the #28 region [Figure 3a]. The growth was tender, firm inconsistency, and not indurated on palpation. Hard-tissue examination revealed a buccoverted, grossly decayed 28 impinging, and traumatizing the growth [Figure 3b]. Based on the history and clinical findings, the patient was provisionally diagnosed with traumatic fibroma of the left buccal mucosa in relation to the #28 region. The preliminary examination was performed, and #28 was extracted, followed by an excisional biopsy of the lesion. Histopathological examination of soft tissue revealed dense fibrous tissue in the subepithelium with capillaries.
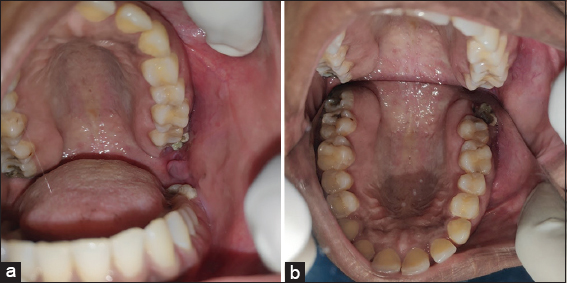
Figure 3: (a) Traumatic fibroma ofleftbuccal mucosa. (b) Buccoverted grossly decayed 28 traumatizing the left buccal mucosa visualized in palatal mirror
Case 4
Mucocele
A 23-year-old male presented with a chief complaint of swelling in the inner side of the lower lip for 1 month. The patient gave a history of accidentally biting the lip while having food before the onset of swelling. The swelling was not painful, and it was initially small, and it has progressed to the present size. On examination, there was a solitary diffuse swelling of approximately 1.0 cm × 1.5 cm was seen in the lower labial mucosa corresponding to #32, #33 region [Figure 4]. The swelling was nontender and soft inconsistency. A provisional diagnosis of mucocele of the lower labial mucosa was made based on the history and clinical findings. Following basic tests, an excisional biopsy of the lesion was conducted under local anesthetic, and the histological findings were congruent with mucocele.

Figure 4: Mucocele of lower labial mucosa
Case 5
Angina bullosa hemorrhagica
A 45-year-old female had the main complaint of a sudden reddish swelling on the left side of the tongue from a day earlier. The patient gave a history of hard food intake before the onset of the lesion. The patient had no bleeding disorders in the past, and there was no history of recurrence of such swelling. On examination, a red-colored blood-filled blister of about 1 cm in diameter was present in the left lateral border of the tongue [Figure 5]. On palpation, the lesion was sessile, nontender, and soft in consistency. The provisional diagnosis of angina bullosa hemorrhagica (ABH) was made based on the clinical appearance and history of the reddish swelling on the tongue’s left lateral border. Laboratory evaluation of complete blood count and coagulation profile did not reveal any underlying disease and gave a normal picture. The healing was uneventful as it ruptured spontaneously within a day. Topical oral steroids and anti-inflammatory agents were prescribed for symptomatic relief.

Figure 5: Angina bullosa hemorrhagica of left lateral border of tongue