CASE REPORT
A 17-year-old female patient approached the department of oral medicine with the chief complaint in the right lower jaw for the past year. She reported a history of sudden onset of swelling, which was initially peanut in size, consequently increased to present magnitude. There was no history of pain, fever associated with swelling. Previous medical, dental, and family history was noncontributory. Extraoral examination revealed asymmetry in the right lower one-third of the face due to diffuse solitary swelling of size 2 cm × 2 cm, roughly oval in shape, extending anteroposteriorly from 2 cm
posterior to symphysis 1 cm anterior to the lower right side angle of the mandible. On palpation, mild paresthesia on the right side mandibular premolar region was noticed. On intraoral examination [Figure 1], a grossly decayed tooth of #46 was detected with a positive note of tenderness on vertical percussion. There was a solitary diffuse irregular swelling in lower right mandible vestibular region which is of size 2 cm × 2 cm extending anteroposteriorly from distal aspect of #44 to mesial aspect of #47. Superiorly from the crest of the alveolar bone to the buccal vestibule inferiorly from #44 to #47. Mucosa over swelling has no color changes. On palpation, there was buccal cortical plate expansion from #44 to #47 and lingual cortical plate expansion in relation to #46. Eggshell crackling was seen on the buccal aspect in relation to 46 region.

Figure 1. Intraoral swelling
According to clinical findings and observations, provisional of periapical cyst of #46 was given with differential diagnosis of ameloblastoma, dentigerous cyst, calcifying epithelial odontogenic tumor (CEOT) and central ossifying fibroma. The patient was addressed to the radiology department where intraoral periapical (IOPA) radiograph of #46 tooth (IOPA), mandibular right lateral occlusal radiograph, and orthopantomography were taken. IOPA revealed dental caries involving pulp region with loss of distal half of coronal part of #46 was noticed. There was a diffuse radiolucency at periapical region extending from distal half of radicular portion of #45 tooth to distal aspect of #47 tooth running peripherally with sclerotic border, which was visible at the apical region of #45 tooth with evidence of internal septa in #45 and #46 interdental regions.
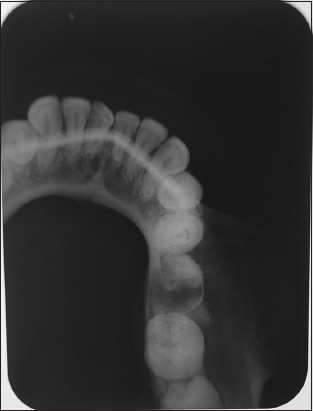
Right lateral mandibular occlusal radiograph depicted buccal cortical plate expansion from #44 to #47 tooth region with the internal structure of mixed radio-opaque and radiolucent structure intermingled with multiple internal septa [Figure 2]. Orthopantamograph revealed solitary well defined, round, multilocular, a mixed radiolucent-radio opaque lesion in right lower mandibular region extending anteroposteriorly from #44 to #47 tooth region apically and superior-inferiorly from the alveolar crest to lower border of the mandible. The mixed

Figure 2. Orthopantamograph
lesion contained many internal septa granting multilocular pattern and displacing the mandibular canal inferiorly. Loss of coronal portion with radicular remnants in relation to #36 was noticed. Radiographic diagnosis of central ossifying fibroma with a differential of multilocular ameloblastoma, CEOT, central hemangioma was recommended [Figure 3].
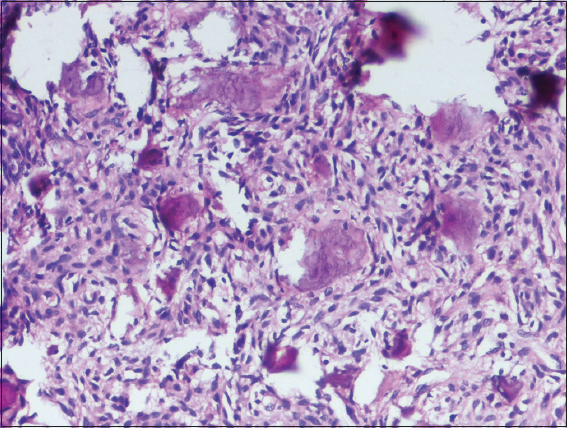
Fine-needle aspiration was performed to find internal content of swelling where the drawing was negative. The patient was subjected to incisional biopsy, the histopathological examination revealed the underlying hypercellular connective tissue of proliferating spindle to fusiform fibroblast arranged in a haphazard manner with discrete deposition of immature bone arranged in a spherical, crescent-shaped like psammomatoid manner and few are in trabecular form with osteoblastic rimming and osteocytes within it, arriving at the diagnosis of psammomatoid juvenile ossifying fibroma [Figure 4]. Bearing in mind, the size and aggressiveness and recurrence rate of the lesion segmental resection was planned and carried out.