CASE REPORT
A 37-year-old woman reported to the department with a chief complaint of replacing her missing teeth in the lower front tooth region of the jaw. Her past dental history revealed that she had undergone extraction of her mobile teeth before 1 year. The patient is a known diabetic for the past 2 years and under control. A detailed family history was obtained, and it was unremarkable.
Clinical examination revealed the presence of all teeth except the lower left mandibular incisor. Miller’s[7] Grade II mobility with a clinical attachment level of 6 was evident in the right lower central incisor. On probing, there was a generalized pocket depth of about 4–7 mm, and she had a score of fair on oral hygiene examination.[8] On examination of the gingiva, there was generalized roundening of the marginal gingiva and ballooning of interdental papilla was evident. Radiographic examination revealed generalized horizontal bone loss.
The treatment plan was aimed at improving the patient’s overall periodontal health as well as to restore the lost tooth. A thorough clinical and radiographical examination revealed Siebert[9] Class III ridge deformity [Figure 1] and further examination revealed that the patient’s palate had sufficient thickness to serve as a donor site.

Figure 1: Preoperative photographs
Hence, ridge augmentation was planned for periodontal prosthesis as the fixed prosthesis is not feasible for the patient due to periodontally compromised teeth. Furthermore, the patient was not opting for the extraction of mobile teeth as well as the implant. Free gingival graft (FGG) itself fulfills the necessary requirements for periodontal prosthesis.
Hence, considering the technique sensitivity for connective tissue graft procedure compared to FGG, FGG was preferred. FGG along with hard-tissue substitutes such as xenografts was planned for ridge augmentation in the edentulous site.
Phase I therapy comprising of scaling, polishing, subgingival root planing, and correction of occlusal disharmony had been followed and revaluated for 4 weeks. In the surgical phase, convention flap surgery was carried out in all the four quadrants in stages, followed by which the soft- and hard-tissue augmentation was carried out.
After administering 2% lignocaine (1: 80,000) (Lignox 2% A Indoco, India), horizontal incisions were given on the lingual aspect of edentulous site 2 mm apical from the crest of the ridge [Figure 2]. Horizontal incision is joint with the sulcular incision extending to 32 and 41, and a full-thickness flap was elevated [Figure 2]. A FGG measuring about 8 mm × 7 mm × 6 mm was obtained from the upper right palatal region. Then, the xenograft (Advanced Biotech Products [P] Ltd.,) particles were placed, followed by the FGG acting as a membrane in the recipient site and secured by suturing (Johnson and Johnson Pvt. Ltd., India) with the flap, and the flap was approximated with interrupted sutures (Johnson and Johnson Pvt Ltd., India) [Figure 3].
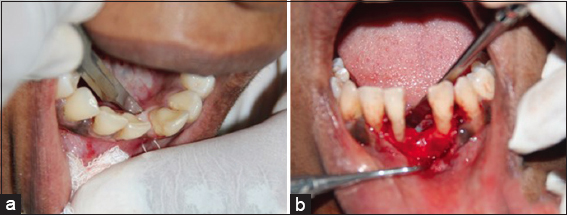
Figure 2: Incision placement and flap retraction

Figure 3: Graft placement and suture placement
Follow-up was done after 1 week, 4 weeks, and 3 months. At the 3rd-month review, a considerable gain in the ridge both apicocoronally and buccolingually was obtained [Figure 4]. After 3-month follow-up, splinting with preimpregnated fiberglass ribbon (EverStick® C and B; GC EUROPE N.V., Leuven, Belgium) along with replacing 31 using flowable composite tooth through indirect method was done where 43, 42, and 33 were used as abutment for stabilizing the periodontally compromised teeth [Figure 5].

Figure 4: Postoperative at 3 months
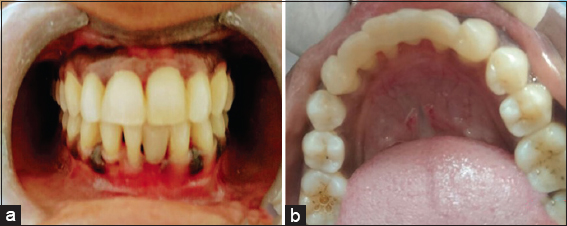
Figure 5: Fiber-reinforced splint along with indirect method of composite tooth placement