INFLUENCE OF CUSPS AND FOSSAE ON DIRECTION OF OCCLUSAL FORCES
A healthy mouth is maintained in the best condition by relating cusps to condyles so that neither one adversely influences the other producing any type of havoc. Occlusal anatomy, however, complex it might appear to be, every complexity has a purpose of its own and a reason to be there. A restorative dentist must respect these complexities and the role they play in maintaining harmony in the overall system. While placing a restoration, a dentist must make an effort to create an occlusion that best suits with the oral environment. Cusps need to be properly placed in the interarch space and must be properly graded in heights and sizes to be in harmony with the movements of the mandible.[3] Optimal occlusion is that which is comfortably adapted by the patient. Therefore, a restoration is designed in a manner that it does not produce any disturbance in the normal condylar path. The magnitude and direction of load borne by the tooth is influenced by its occlusal anatomy.
In posterior teeth, the occlusal morphology is reproduced in a fashion that during mandibular closure there are even simultaneous contacts of maximum possible teeth achieving (a) maximal stability of the teeth (b) minimizing the amount of force placed on each tooth in function. The contact pattern of the teeth should be such that it directs the occlusal forces favorably for their adequate dissipation.
The tooth is housed in a bony socket with intervening periodontal ligament. The osseous tissue does not tolerate occlusal forces well; it shows resorption when under pressure. The periodontal ligament contains collagenous fibers that attach the tooth to the bony socket. Under the influence of occlusal forces, the fibers support the tooth, and tension gets created at the point of attachment of these fibers in the alveolar socket. This tension (i.e., pulling) actually stimulates osseous tissue formation. Therefore, a destructive force (i.e., pressure) is converted into a constructive force (i.e., tension) by the periodontal ligament, thereby acting as a natural shock absorber.
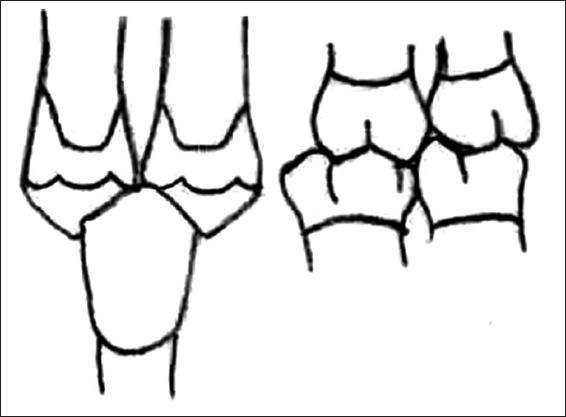
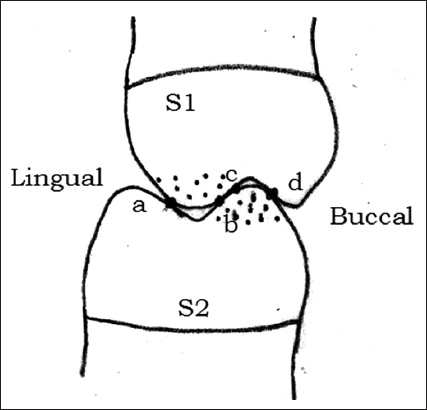
When the occlusal morphology is such that the cusp tip is contacted on a flat surface, i.e. bottom of a fossa or crest of the marginal ridge, the resultant occlusal force gets directed vertically along the long axis of the tooth. The fibers of periodontal ligament are arranged in a manner that such forces are well accepted and dissipated [Figure 1].

Figure 1: Cusp-fossa contact. Occlusal force (v) directed vertically along the long axes of teeth. Uniform tension (T) seen in periodontal ligament fibers
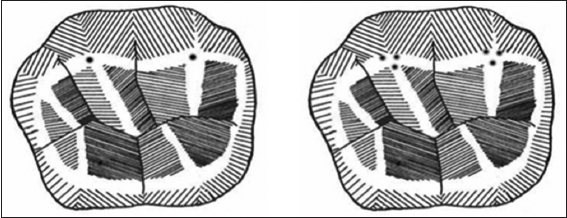
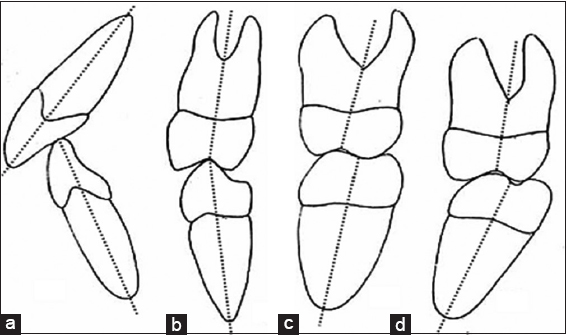
As opposed to this, when the occlusal morphology is such that the teeth contact each other on an incline, the resultant force is not directed along the long axis, instead a horizontal component is created which tends to cause tipping of teeth. The fibers of the periodontal ligament are not properly aligned to control them. On tipping, some fibers get compressed while others get pulled. Overall the forces are not effectively dissipated to the bone which can result in a pathological response of the bone in the form of resorption [Figure 2]. A neuromuscular reflex response may also be created in an attempt to avoid the incline contacts.[3,4] Improperly generated forces during incline contacts can have adverse influences such as tooth fracture, tooth jiggling, or mandibular deflection [Figure 3].[5]
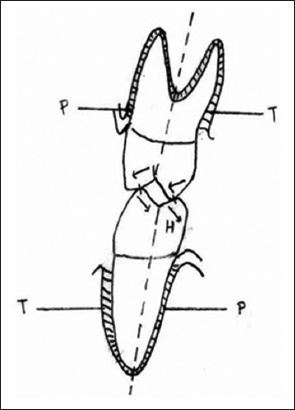
Figure 2: Cuspal incline contact. Horizontal component (H) of occlusal force created causing tipping of teeth. This tends to cause compression (P) and tension (T) in the periodontal ligament

Figure 3: Clinical Consequences of incline contacts (a) cuspal fracture, (b) tooth jiggling, (c) mandibular deflection