CASE REPORT
A 34-year-old female presented with a painless, submucosal, movable mass in the soft palate which was present since 3 months. The mass was located in the left posterior palatal region, measuring about 2 cm × 1.5 cm in size with a distinguishable boundary [Figure 1a]. The mass was oval in shape, firm in consistency, and nonpulsatile in nature with overlying mucosa normal in color and texture. There was no complaint of paraesthesia. The clinical features simulated a benign lesion, and so an excisional biopsy was planned. A signed informed consent was taken from the patient for the surgical intervention which was performed keeping a safe margin of 0.5 cm [Figure 1b].
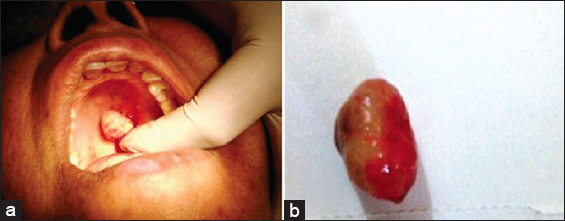
Figure 1: (a) Clinical presentation of keratocystoma of the palate. (b) Resected specimen of keratocystoma
Macroscopically, the cut surface of the excised mass demonstrated multilocular cystic spaces showing grayish brown solid areas. Histologically, the section showed a benign tumor with multicystic spaces and focal solid epithelial cells lined by benign squamous epithelial cells but without lobar architecture [Figure 2a]. The overlying epithelium was parakeratinized and without a granular layer. Cells had abundant eosinophilic cytoplasm with bland, uniform nuclei [Figure 2b]. The cystic spaces were filled with keratin material. These findings helped us to reach a provisional diagnosis of keratocystoma. However, keeping in mind the rarity and uncertain behavior of this lesion and to confirm the diagnosis, we went for advanced immunohistochemical study with a panel of markers (high molecular weight cytokeratin, cytokeratin, p63, and MiB-1). On IHC examination, the tumor cells were found positive for HMWCK, focally for CK7, CK19, and p63 and Mib-1 labeling was approximately 1% [Figure 3a-c]. Furthermore, focal foreign body giant cell reaction to the keratin material was visible. The histological and IHC findings were consistent with those of keratocystoma which suggested of a diagnosis of keratocystoma of the palate.
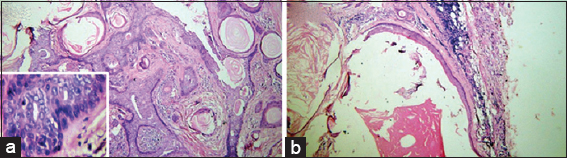
Figure 2: (a) Photomicrograph showing multicystic spaces and numerous keratin pearl like areas (H and E stain, ×10); Inset (×40) showing cells with eosinophilic cytoplasm and bland uniform nuclei. (b) Photomicrograph showing parakeratinized cystic lining and epithelium (H and E stain, ×10; scanner view)
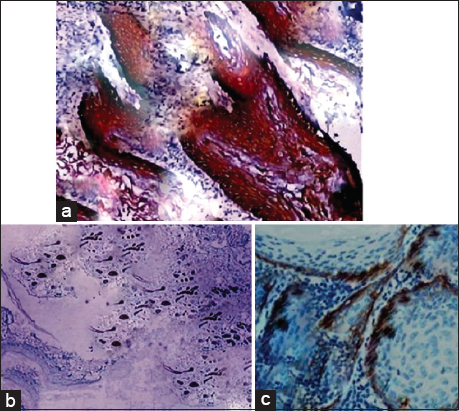
Figure 3: (a-c) Immunohistochemical findings of specimen. (a) Tumor cells are positive for HMWCK. (b) Focally for CK7 and (c) p63